

I begin by paraphrasing Indian Prime Minister Narendra Modi’s address to the nation on March 14, 2020 on the novel coronavirus (COVID-19) outbreak. It was an appeal to put our health first on our priorities to ensure that the world is healthy. It had the solemn message of service as the highest duty in the time of crisis.
He said that we cannot feel everything is alright since the COVID-19 pandemic, a disease which has no vaccine and no cure, has affected more countries than both the great wars. Countries have made efforts to isolate and citizens have cooperated. India with a 1.3 billion population is a developing nation— the time and challenge of pandemic are extraordinary. We shall be affected as the globe is affected. Two main things required to fight the challenge— “Sankalp” and “Sanyam” (commitment and restraint).
Every citizen must follow his/her civic duty— we shall avoid getting infected and save others from infection. He exhorted the citizens not to go to crowded places, not to go out of home— social distancing is most essential and useful. Overconfidence and hubris that nothing will happen to us is misplaced- it is an injustice to others. Work from home. All senior citizens (above 60) should remain isolated at home.
He requested people not to load the hospitals— no routine checks and postpone elective surgeries— to de-stress medical systems.
He informed the nation of the constitution of a COVID-19 economic task force, which will be in touch with all stakeholders, and will decide in near future on steps to mitigate economic stress and ensure all steps are seriously implemented.
He made an appeal to all rich people to take care of the economic interests of all these service providers, to give them full salary since they must take care of their families.
He assured Indians that there shall not be shortage of milk, food, medicines. All steps are being taken to ensure supply does not stop. He appealed not to hoard essential commodities.
India was to voluntarily “situate-in-place” on Sunday, March 22, in preparation for a long haul of restrictions and containment in our fight against the virus.
It was an appropriate, concise and relevant appeal covering all essential areas where a battle needs to be mounted in the ongoing war against the novel coronavirus outbreak.
The community spread of COVID-19 in India has not started, according to authorities. About 80 districts and a dozen states have gone into lockdown, which is an expeditious preventive step to stop the virus from spreading in community. This will surely lead to breaking the chain of transmission.
In countries, where community transmission has reared its head, health systems have crumbled, markets have crashed, and unemployment has peaked to unprecedented level. Global economic recession is inevitable due to disruption of supply chains, manufacturing and employment.
This paper presents a COVID-19 combat strategy for India based on examination of facts on the disease, strategies of different nations which have proved successful in containment, and scientific research which offers reasonable models for future course of the epidemic. It suggests how may we use our existing disease surveillance systems, disaster control and command logistics along with our unique strength as a community to contain the epidemic without considerable loss to lives and livelihoods. We clearly understand that the pandemic is not only a major global health crisis but is also a major labour market and economic crisis. So, we also look at economic and geopolitical considerations for India.
Situation Report
As I file this report, India reports a total of 396 confirmed cases of COVID-19 and 7 deaths.
Covid-19 Real time
Covid-19 India
For detailed information on Corona virus please see WHO-China Joint Report
A quick comparison with Italy
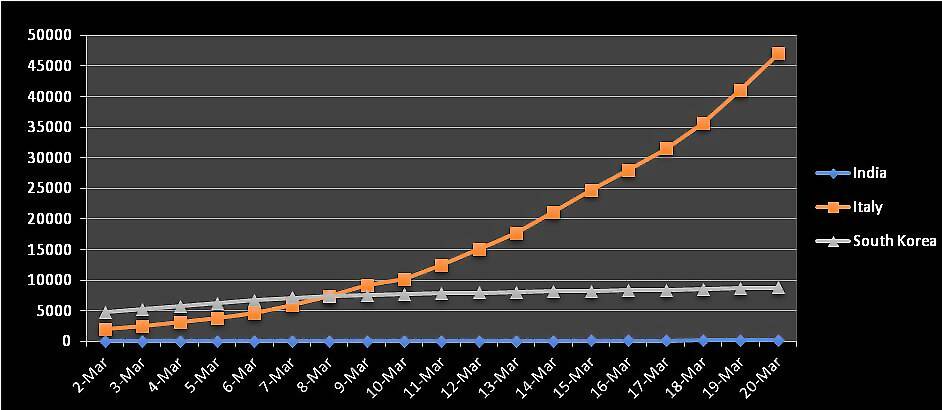
If we strike preemptively, we are surely not going the Italy way. Data suggests direct comparison of COVID-19 scenario and progression in India with Italy is not warranted. Italy has the second largest geriatric population in the world, with average age of corona related deaths being 81. The healthcare system is mostly single-tiered with direct admissions to emergency care in normal times, and thus everyone from mild to severe cases loaded on to tertiary facilities, leading to unenviable triage and selection of sick people for prioritisation of treatment leading to many deaths. Moreover, it is directly on the China Silk Route with direct connectivity to Wuhan. It was a little late in preventing entry of the contagion, and the result is apparent. Lastly, the people greet with physical contact and kissing as part of the culture, turning the entire society into a petri dish for viral propagation.
The following chart compares epidemic progression in March, 2020 for India, South Korea and Italy, clearly showing the vast gap in cases reported and resulting casualties. It also reflects South Korea’s success in mitigation and control with contagion stabilizing over the past week.
Figure 1: Covid-19 positive cases in March,2020 in Italy, India and South Korea
Where we stand
Now lets look at incidence and progression in India since the first case was detected on January 30th, 2020 in the following graph-
Figure 2: COVID-19 positive cases and casualties in India since inception (315 cases, 5 deaths on 3/21/02) Live dashboard for the world
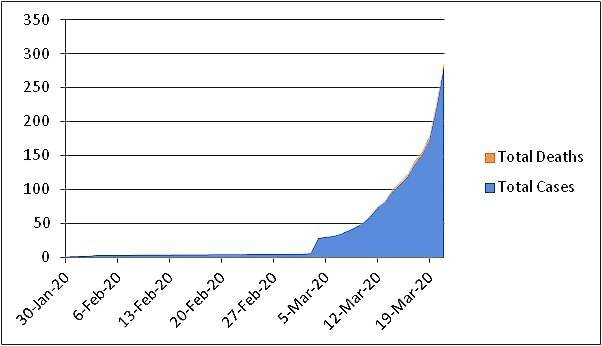
The picture shows the epidemic assuming exponential progression in March with India graduating to stage 2 of the pandemic. However in India, we have not been able to ensure contract tracing resulting in many asymptomatic cases going undetected who are currently moving around and spreading the contagion involuntarily. The death rate obtained from simply dividing deaths with cases is ~ 0.018, much lower than the rest of the world.
Its only on Saturday (March 21, 2020), ICMR has changed the testing strategy to test all symptomatic cases and their direct and high-risk contacts, escalating from testing only symptomatic international travelers. Symptomatic contacts of laboratory confirmed cases, symptomatic health care workers, and all hospitalized patients with Severe Acute Respiratory Illness (fever AND cough and/or shortness of breath) will be tested as well. It is still majorly constrained and may not assist in containing the communal spread.
Following is the most important chart to put some realism in above contention that we are testing too little for our effort at mitigation or suppression to be fruitful-
Figure 3: Suppression Strategy in Hubei
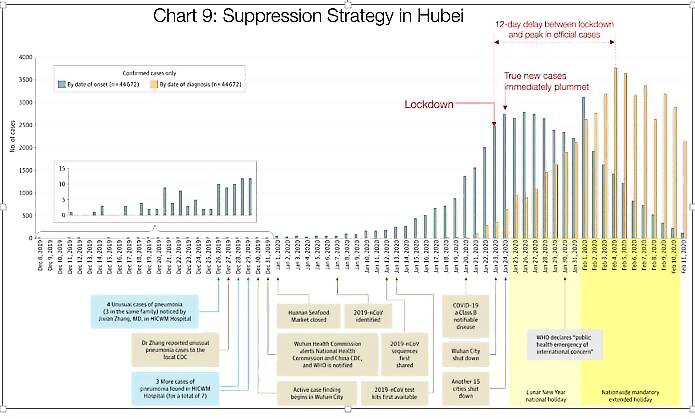
Source: Tomas Pueyo analysis over chart from the Journal of the American Medical Association, based on raw case data from the Chinese Center for Disease Control and Prevention (1)
The orange bars are the confirmed cases through testing, but the grey bars are true cases in the community which predate the official detection by many days, and in absence of movement restrictions spread the epidemic to the proportions we see today. This one graph categorically lays down the need for extensive random testing, mainly in high prevalence areas and immediate need for social isolation at various levels across the country depending on real time tracking of cases and risk assessment. Briefly when the city reported 400 cases, there were in fact 2,500.
With this in background we may now venture to model some future scenarios of epidemic in India.
Best-case scenario
That would be if Indians have an inherent immunity and the virus dies down in ensuing summer heat.
WHO predicts that heat and humidity do not slow down infectiousness and spread of COVID-19. To quote “From the evidence so far, the COVID-19 virus can be transmitted in ALL AREAS, including areas with hot and humid weather.” (Heat won't help)
But a study by MIT researchers provides an evidence to the contrary. To quote “transmission of 2019-nCoV virus might be less efficient at warmer temperatures and therefore with approaching summer temperatures in the Northern Hemisphere, the spread of 2019-nCoV might decline in the next few months.” (Heat may help)
I view of the uncertainty the proof shall present itself in ensuing summer only. Moreover, the second phase in the fall (after summer) may be more severe like 1918 Spanish Flu pandemic if we are not ready with vaccine or treatment by then. COVID-19 has spread in hot climates so far and thus there is little leeway for us to put our guard down and throw caution to wind. Given such unpredictability, Our strategy and preparation must be for the worst-case scenario while hoping for the best.
Worst-case scenario
Department of Homeland Security in US predicts that in a very severe case, 11% of the country's population shall require medical care, 3 % shall require hospitalisation and 0.9% shall require intensive care with ventilators or extra-corporeal oxygenation etc. If we extrapolate the stats to India, that is 152 million requiring medical care, 41.4 million hospitalisations with 12 million in critical care/ICU. (Indian Population- 1.38 billion in 2020) (Live Population)
We may like to look at this dynamic modelling for predicting various scenarios given characteristics of the population, interventions as well as the virus-Epidemic Calculator
How ready are we to handle the worst-case scenario?
We may expect a run on medical facilities when a huge number of people get affected at once. With India’s numbers of population, even small percentages shall generate millions of cases.
Following three figures give a comparison of medical infrastructure and personnel in comparison to countries at front line of fight with COVID-19.
Figure 4: Hospital beds per 1000 population
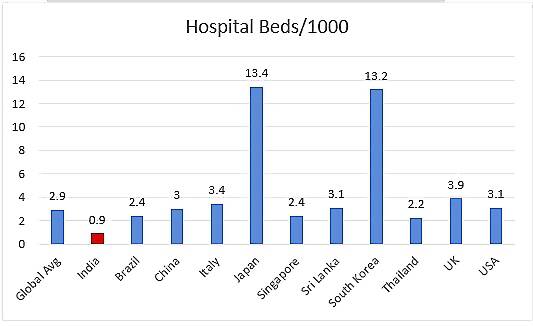
Source: World Bank (Beds/1000 Pop)
Figure 4b: Critical Care Hospital beds per 100000 population
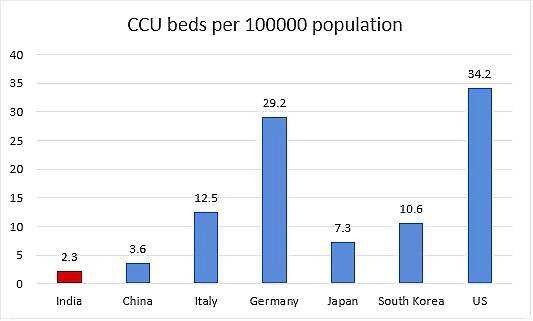
Figure 5: Physicians per 1000 population
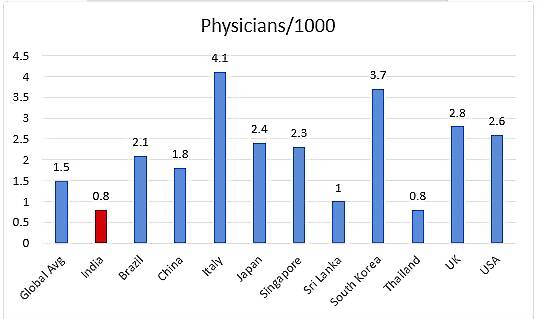
Source: WB (Physicians/1000 pop)
Figure 6: Nurses and midwives per 1000 population
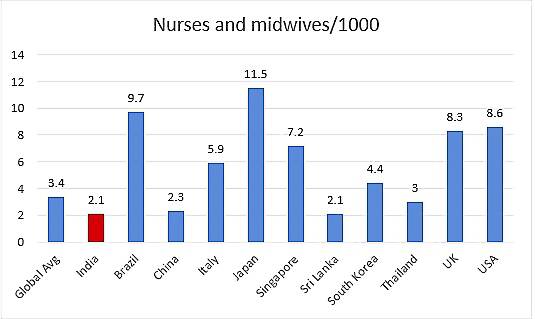
Source: WB (Nurses/1000 pop)
Just a rough estimate of India having 30,000 ventilators is given by Economic Times, with 800 in Mumbai, the worst-affected big city. The prospects for new manufacture are grim given supply line of component parts are closed due to travel ban.
Even the best health systems like that of Italy have crumbled when they faced a run and got overwhelmed due to community transmission leading to a deluge of cases requiring hospitalisation. Given the sitrep, India is least prepared for handling such an outpouring. Hence our best strategy is proactive containment and prevention of community spread.
Recommended strategy
Amid a very unpredictable pandemic scenario, COVID-19 presents us some actionable certainties. First, we know there is no immunity against it and the entire population is at risk of contracting it if exposed. The virus spreads through proximity of infected persons who spread it through aerosols and nasal secretions. It is not airborne. So, we need to be within a metre of an infected person to get the contagion. It can survive on various surfaces for up to 72 hours, and this is a major route of transmission in the community. Aerosol and Surface Stability of COVID-19)
The estimates from different studies show that the virus has an Ro of 2.2 i.e one infected person shall, on an average infect another 2.2 if not isolated. The doubling time of cases is 7-10 days. If containment is not done, it might infect 30-40% of the population, out of which 5% shall require hospitalisations, and 1% ICU care.
COVID-19 outbreaks can be contained, and transmission stopped, as has been shown in China and some other countries.
WHO’s strategic objectives for this response are to:
- Interrupt human-to-human transmission including reducing secondary infections among close contacts and health care workers, preventing transmission amplification events, and preventing further international spread*
- Identify, isolate and care for patients early, including providing optimised care for infected patients
- Identify and reduce transmission from the animal source
- Address crucial unknowns regarding clinical severity, extent of transmission and infection, treatment options, and accelerate the development of diagnostics, therapeutics and vaccines
- Communicate critical risk and event information to all communities and counter misinformation
- Minimise social and economic impact through multisectoral partnerships.
[*This can be achieved through a combination of public health measures, such as rapid identification, diagnosis and management of the cases, identification and follow up of the contacts, infection prevention and control in health care settings, implementation of health measures for travellers, awareness-raising in the population and risk communication. For more information, visit WHO SitReps]
Two fundamental strategies are possible:
(a) mitigation, which focuses on slowing but not necessarily stopping epidemic spread – reducing peak healthcare demand while protecting those most at risk of severe disease from infection, and
(b) suppression, which aims to reverse epidemic growth, reducing case numbers to low levels and maintaining that situation indefinitely.
Mitigation or suppression?
Among the strategies of mitigation vs suppression, it is the latter which has shown clear evidence of containment of epidemic. This strategy has been shown to be extremely effective in China, Taiwan, South Korea and Singapore. China resorted to early totalitarian lockdowns in affected areas. The strategy was to trace and isolate all contacts of confirmed cases which traced 100% such cases as per reports, no small feat in densely populated areas like Wuhan (locked down at 495th case) and Guangzhou (locked down at 7th case; early lockdown ensured medical facilities were not overwhelmed unlike Wuhan). In Wuhan alone there were 1,800 tracking teams with 5 members each to accomplish the task. Chinese State’s complete control over citizen’s data and whereabouts through smart phones made this huge endeavor a success. As of today, China is claiming to have stemmed the tide of COVID-19 with no new cases reported from inside the country.
Taiwan, Singapore and South Korea achieved comparable results by affecting quarantines, isolation and social distancing through beautiful example of community participation, communication, surveillance, social distancing, containment and medical intervention. They educated, empowered and trained communities to achieve exemplary and heartening results in control of the pandemic. (Lessons from Singapore). South Korea went the “test, test and test” way followed by isolation and treatment on the road to success.
We need to keep in mind that fight with this pandemic is a marathon, and we need to come to terms psychologically to face inconvenience in the long haul. That is absolutely essential to flatten the curve and prevent a mortal run on our limited health facilities.
The strategy for India is outlined briefly as follows:
1. Travel Restrictions
These are already in place. Studies show once the virus has entered the community such restrictions are only mildly effective. Only transmission-reduction interventions will provide the greatest benefit to mitigate the epidemic. The restrictions, however, have psychological effect that the government is doing something for the safety of its citizens. (Effectiveness of Travel Restrictions)
2. Social Distancing
To beat COVID-19, social distancing is a must. (Social distancing a must)
We need to stay at home and venture out only in case of essential needs like food and medicines. Avoid gatherings, greet from a distance, wash hands regularly and stay a metre apart from people.
Undetected cases were responsible for 86% of new infections in China, and infections dropped precipitously after social distancing measures were put in place there.
Most parts the nation have now commenced lockdown for about 10 days. We may have to “shelter-in-place” for some weeks: at least 8, going by the current evidence. It may take some months before the virus is contained or a vaccine is developed before we can assuredly abandon precaution and resume life as it was before the inception of the pandemic. Still much would have changed in socio-economic sphere and thoughts about what the world might look on the other side of curve is unnerving to say the least. (A changed world order)
(Lets flatten the curve)
How prepared are Indian citizens to go under lockdown?
The findings of the author on Sentiment Analysis of 12,447 Twitter feeds in India from 10th to 21st March carrying hashtags related to Corona (#coronavirus, #COVID19, #coronaviruspandemic, #coronavirusoutbreak etc.) shows that the sentiment is polarised on the issue with no middle ground. Fortunately, majority show positive sentiments on the issue and are not panicked. We may guess that the citizens are amenable to suggestions of restraints and shall refrain from hoarding of essential food supplies and medical equipment. Such optimism may also allow us to face the economic crisis with fortitude, provided the government is able to sustain the consumer sentiment through announcements on financial aid, wage security, tax and mortgage relaxations and cut in interest rates.
Figure 7: Sentiment Analysis of Twitter feeds around Corona Virus in India- 1 is very negative, 5 is very positive.
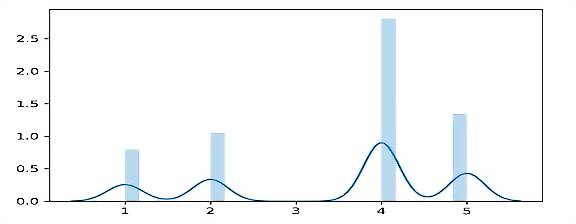
The scale is from negative to positive starting from 1 from 10 to 20th March 2020. It’s the time around Prime Minister’s address to the nation on coronavirus. The mood of the people seems positive and upbeat giving hope that India as a community shall put up a disciplined and sustained fight to counter the pandemic as well as economic challenges.
3. Test, Track, Treat and Isolate: Surveillance and response
Director General WHO has given a singular clarion call to nations to “test, test and test”. India is just not testing enough!
Prioritise active, exhaustive case finding and immediate testing and isolation, painstaking contact-tracing and rigorous quarantine of close contacts.
We have an extensive system of surveillance in the country under vertical disease control programmes like National Tuberculosis Program. The net of National Health Mission is extensive and its reporting systems robust. We may press the surveillance systems in practice for keeping a close watch on evolution of COVID-19 in the country. Expand National Communicable Disease Surveillance Programme, NIC’s Disease Outbreak Monitoring Call Centre and Influenza Surveillance Networks but they must essentially report to a single agency.
IDSP (Integrated Disease Surveillance Programme) may act as the nodal agency for syndromic reporting. NCDC may report to it in place of working parallelly. We already have notified helpline numbers and email addresses for communicating with public. Any report of suspected case must be investigated, tested and its contacts traced for quarantine and isolation.
At the grassroots, ANMs and ASHAs may be trained to identify and report suspected cases for further necessary action, and to communicate with local public on importance of social isolation and other suggested measures announced by the government.
We also need to keep a close watch on food security and maintenance of essential services across the nation with active involvement of local bodies.
4. Map and engage Health infrastructure and personnel at all levels
We need to map medical facilities, availability of beds, personnel and equipment including critical care- both public and private and requisition necessary reservation to meet surge capacity in demand for treatment of COVID-19 cases in eventuality of it spreading on large scale.
It is better to be prepared in advance when the course of the disease is largely a guessing game.
It is suggested that quarantine and isolation, which require high degree of discipline and monitoring(given many instances of patients running away from hospitals) may be placed under Director General Armed Forces Medical Services (DGAFMS), with Ministry of Health and Family Welfare providing all logistic support when required.
5. Stock PPE and other essential supplies
Doctors and nurses have made fervent appeals for adequate provision of Personal Protective Equipment (PPE) to governments in countries facing big surges in COVID-19 infections, with some having died when constrained to deal with patients without adequate protection. Some months back, such a scenario would have sounded surrealistic to almost all, but now world is facing such a reality and struggling to cope with it.
To ensure enough and steady supply of PPE, ventilators and other critical care equipment, tubing, essential drugs, disinfectants etc. to our first responders in the field and medical community we need to assess installed capacities for manufacture and stockpile all of these commodities or meeting surge demand, modelling for worst case scenario. With the world in a lockdown and supply chains blocked, we must essentially rely on our own capacity to manufacture the items.
Even if we face a mild outbreak, these stocks can be used later.
It is also an apt time to reclaim our self-reliance in manufacturing APIs for essential drugs and laboratory regents for testing. There are reports of high throughput systems of test manufacturers running out of regents, and that may severely retard our already meagre capacity of testing.
There is a need for wartime urgency to amp manufacture of masks, respirators, ventilators, sanitisers, hazmat suits etc. like the UK who have engaged private manufacturers of cars and luxury goods to produce essential medical equipment.
6. Risk Communication and Community Engagement (RCCE)
“Proactively communicate and promote a two-way dialogue with communities, the public and other stakeholders in order to understand risk perceptions, behaviors and existing barriers, specific needs, knowledge gaps and provide the identified communities/groups with accurate information tailored to their circumstances. People have the right to be informed about and understand the health risks that they and their loved ones face. They also have the right to actively participate in the response process. Dialogue must be established with affected populations from the beginning. Make sure that this happens through diverse channels, at all levels and throughout the response.” -WHO (WHO RCCE Guide)
It is also essential to communicate with citizens to curtail rumors and allay apprehensions and anxiety due to uncertainty in the situation.
7. R&D
A freely available dataset CORD-19, which is a resource of over 44,000 scholarly articles, including over 29,000 with full text, about COVID-19, SARS-CoV-2, and related coronaviruses is provided to the global research community the White House and a coalition of leading research groups. (CORD-19 data)
Since not much is known about the novel virus, Indian medical research institutions may take up the research in collaboration with WHO and other agencies to establish facts on viral transmission routes, disease progression, disease course, immunity, vaccination and therapeutics of the novel coronavirus. Besides adding to the global knowledge, it shall help India to fine tune the response and plan better. (WHO R&D Guide)
Now I discuss four topics in some detail-
1. How to keep people gainfully engaged while situated at home.
2. Solidarity clinical trial of WHO for finding a cure.
3. Economic measures to combat recession.
4. Geopolitical cooperation
Combatting Cabin Fever: How to keep people gainfully engaged while sheltered in place
Social distancing, isolation and quarantine being vital to stop the transmission of COVID-19 transmission, prolonged stays at home are inevitable. While disrupting the work and educational engagements of millions, it might induce affective and psychological distress if younger and active people are not gainfully engaged. People may face a range of negative feelings, distress related to restricted movement, irritability, boredom, some hopelessness, restlessness and difficulty concentrating.
While work places and schools might be putting in place a slew of measures to continue activity online or remotely, people are going to rely heavily on visual media and social-media platform for news and entertainment as well as for keeping in touch with their loved ones.
This is an appropriate time for departments of education and educational boards to put uniform online curricula for all classes for students sitting at home. Such courses are hugely popular on platforms like MOOCS, Coursera and Khan Academy; but are not adjusted to the Indian school system.
On the same line, agencies like Skill India may host short vocational training certification programmes online and may also enable online interactions of learners with experts for learning to be effective.
The content generated once shall help us in perpetuity.
Data may be subsidised under corporate social responsibility measures of telecom providers so that citizens remain connected and informed through the crisis.
There is also a downside to increased engagement on internet.
Studies show that volume of WhatsApp and Facebook Messenger calls has doubled in the last one month whereas Instagram and TikTok show 22-27% increase in activity.
Such traffic may lead to run on internet services which might break. European Commissioner Thierry Breton has requested streaming platforms like Netflix to switch to standard definition when HD is not necessary.
Further, unhindered social media content and misinformation has the potential to derail all well-meaning government steps to combat the pandemic and allay the fears. (Social media and misinformation) WHO has warned of such an “Infodemic” of rumors which it defines as “an overabundance of information—some accurate and some not—that makes it hard for people to find trustworthy sources and reliable guidance when they need it.” It has exhorted governments to actively counter such rumors and myths which might derail genuine efforts at control and cure of the virus. (WHO on Infodemic)
Facebook, Twitter, and YouTube all announced this week that thousands of content moderators are being sent home—leaving more of our feeds in the hands of machines. Government agencies need to engage directly with the people and ensure that only verified content is fed through regular media so that people do not fall prey to misinformation, jeopardising their own health and derailing public efforts to fight the disease. Such posts have resulted in run on markets and unnecessary hoarding of commodities especially masks and sanitisers resulting in their shortage to health care providers. (How to fight infodemic)
Clinical Trials for COVID-19 vaccine and therapeutic agents: WHO Solidarity Trial
“That’s the creative juice we need right now, as we try and take care of these patients literally on the run”- Dr. Schacher, University of Minnesota
Director General of WHO was not misplaced in calling the event of a vaccine for COVID-19 going for trial just two months of revelation of its genome. As of today, 20 candidate vaccines have gone on trial across the globe. It might still be a long time before a vaccine is launched for mass consumption, and thus the need for strict non- therapeutic measures to control spread is reiterated.
WHO has also launched an extensive multi-country clinical trial for testing the efficacy of clinical interventions and therapeutic agents to jumpstart research on finding a cure for the virus. To date, Argentina, Bahrain, Canada, France, Iran, Norway, South Africa, Spain, Switzerland and Thailand have confirmed that their participation.(Solidarity trail) This trial has five arms-
-Trial on Standards of Care- Study of recommended and used supportive and ancillary measures to combat the disease in hospitalized patients
-Use of anti-viral drug Remdesivir (1)
- Use of anti-viral drugs Lopinavir and Ritonavir (2)
- Use of anti-viral drugs Lopinavir and Ritonavir with Interferon β- an immune-modulator drug
- Use of Chloroquin and Hydroxychloroquin, anti-malarial which have shown promise in inhibiting the virus in laboratory settings.(3)
Besides these some other drugs like Losartan which is an antihypertensive have gone into trial in US.(4)
(The references are to scientific papers on trials of these drugs in cure of COVID-19)
Given the technological and logistic edge of India in vaccine development and production, it came as a surprise that there was no announcement of an effort to develop a COVID-19 vaccine from the country. Indian physicians at Jaipur’s SMS Hospital claim to have treated three patients with a combination of two anti-retroviral drugs and anti-malarial Chloroquine. Despite the government endorsing the claim, no formal clinical trials have been launched. May be the disease was thought of as an imported malady likely to mitigate without transmission in India. However, we are still in time to study the local characteristics of the virus in India, whether it has mutated and examine development of a vaccine. Given our logistic and cost advantages, we might be able to lead the world effort in this regard while not falling behind in our attempt to help the humanity at the time of an unprecedented challenge.
It is a good time for India to join the WHO trial for finding the treatment of COVID-19. We may also utilize the time to test therapies and drugs of AYUSH while following the clinical and ethical guidelines for such trials.
Further the operational research for tracking the contacts and presumptive cases and decisions on curfew and containment need to be taken on real time basis using GIS, GPS, mapping, vulnerability assessment through risk analysis and predictive modelling needs to be put in place. Some steps in this regard like geo-fencing of suspected cases, seem to be already in place and need prompt scaling up at the national level. (News in Hindu)
Fighting the pandemic of inevitable economic recession
“This is no longer only a global health crisis; it is also a major labor market and economic crisis that is having a huge impact on people."
Guy Ryder, ILO’s Director-General
Experts are unanimous in their assessment and prediction of worldwide recession in face of the COVID-19 pandemic. While the pandemic is foremost a public health emergency it is likely to depress global GDP growth to below 2.5%- the threshold for recession for world economy.
UNCTAD’s director of globalisation and development strategies, Richard Kozul-Wright says “No one saw this coming – but the bigger story is a decade of debt, delusion and policy drift.” A combination of asset price deflation, weaker aggregate demand, heightened debt distress and a worsening income distribution could trigger a more vicious downward spiral. (UNCTAD Report)
Global and local supply chain disruptions are inevitable, so is the depression in demand and investment.
Figure 8: Global GDP Growth, 1995-2020
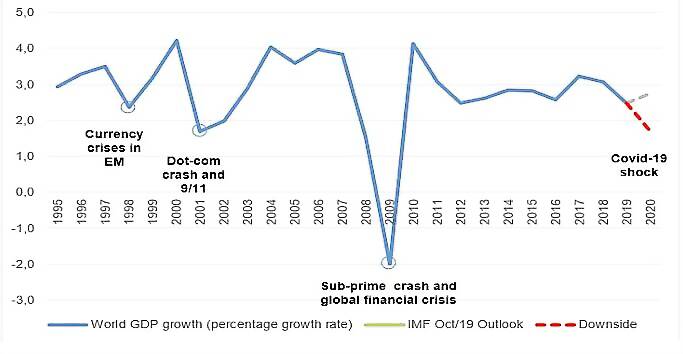
Source: UNCTAD calculations based on IMF, WEO, October 2019
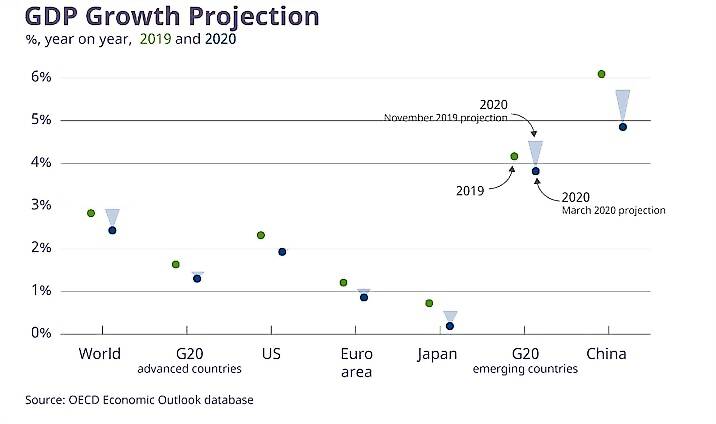
Figure 9: Global GDP Growth projection 2020
The crisis has already transformed into an economic and labour market shock, impacting not only supply (production of goods and services) but also demand (consumption and investment). Based on different scenarios for the impact of COVID-19 on global GDP growth preliminary ILO estimates indicate a rise in global unemployment of between 5.3 million (“low” scenario) and 24.7 million (“high” scenario) from a base level of 188 million in 2019. The “mid” scenario suggests an increase of 13 million (7.4 million in high-income countries). Though these estimates remain highly uncertain, all figures indicate a substantial rise in global unemployment. For comparison, the global financial crisis of 2008-9 increased unemployment by 22 million. (ILO Report)
The crisis is most likely to adversely effect small and medium enterprises (SMEs), and workers in casual and daily wage employment in the informal sector, which NITI Aayog estimates as 81% of all employment in the country . The wages and working hours are likely to be adjusted downwards across leading to increased poverty and depression of demand.
The investor and consumer confidence are already showing signs of depression. Governments need to actively interfere and ensure financial security as appeals to good sense of businesses themselves at the verge of closure due to insidious effects of pandemic may not work.
As witnessed in previous crises, the shock to labor demand is likely to translate into significant downward adjustments to wages and working hours. While self-employment does not typically react to economic downturns, it acts as a “default” option for survival or maintaining income - often in the informal economy. For this reason, informal employment tends to increase during crises. However, the current limitations on the movement of people and goods may restrict this type of coping mechanism. (ILO Report)
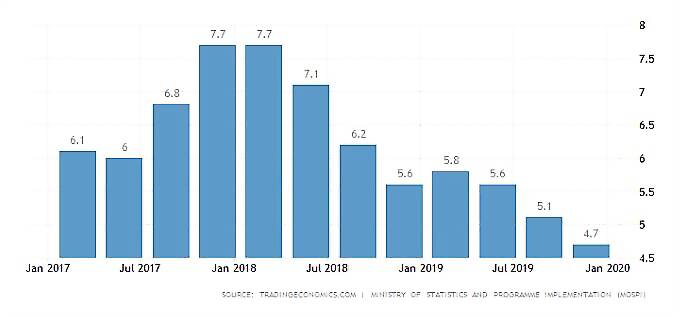
Figure 10: India’s GDP Growth over last 12 quarters
OECD Interim Economic Outlook Forecasts of March 2, 2020 has adjusted India’s forecast downward by -1.1 from November 2019 forecast for the year 2020 pegging it to 5.1%, whereas for 2021 it is adjusted downward by -0.8 to 5.6%. (OECD Report) Like the rest of the world, India is also looking at long term adverse effect of the pandemic on economic growth.
Taking cues from many countries which have put in place immediate measures like cutting interest rates and announcing financial packages to address imminent recession and consequent unemployment, India’s ministry of finance needs to act promptly in announcing a slew of confidence building fiscal and monetary measures. This is a great time to put some cash in the hands of Indian public who are not only facing immense uncertainty on the health front but are directly glaring at widespread loss of livelihoods and dip in incomes. The financial inclusion steps taken by the government in the recent past shall come in handy at this time. Most vulnerable populations like casual workers, daily wagers, informal sector workers especially need to be covered, and the steps need to converge with assurance of food security to their families.
Wage subsidies need to be provided to MSMEs to enable them to keep workers on the payroll. For the middle-income groups, temporary rebates in income tax and mortgage relief may be looked at. These may be back-loaded over time after the crisis is over if our revenues do not allow complete waivers.
Fiscal and monetary easing is the call of the hour and its prompt announcement shall give much needed security and confidence to millions of workers and their families in the face of grave concern and uncertainty the pandemic has presented. At the same time government must engage in constructive dialogue with all stakeholders like industry groups, labour unions and social organisations to allay their fears, address their concerns and extend immediate help as and when required.
Lending and financial support to critical sectors especially health to provide health access to all is the need of the hour. In this unprecedented time, we need to work together, work with fortitude and keep our spirits and confidence high.
For reading further details on status of current economy, please see Economics in time of COVID-19
Geopolitical engagement and regional leadership
We have seen China manoeuvre very quickly in the geopolitical space conceded by the US due to its delayed realization and steps to counter the disease. While US and other developed nations are still weighing containment strategies, and allow an uneven response across regions, China has clearly emerged as the Country the world is looking up to for guidance, aid and assistance in fighting the pandemic. When no European state answered Italy’s urgent appeal for medical equipment and protective gear, China publicly committed to sending 1,000 ventilators, two million masks, 100,000 respirators, 20,000 protective suits, and 50,000 test kits. China has also dispatched medical teams and 250,000 masks to Iran and sent supplies to Serbia, whose president dismissed European solidarity as “a fairy tale” and proclaimed that “the only country that can help us is China.” Alibaba co-founder Jack Ma has promised to send large quantities of testing kits and masks to the United States, as well as 20,000 test kits and 100,000 masks to each of Africa’s 54 countries. (Corona Virus could reshape global order)
In previous global crises like 2008 financial crisis and 2014 Ebola epidemic- the US led the global fight whereas the current US seems to have abdicated the role by looking completely inwards. It has faltered there as well. A global political leader draws the authenticity for its rule through legitimacy of its governance, freedom of its institutions and an inclusionist and benevolent policy outlook. India enjoys such legitimacy and scores over China in this regard.
With China’s offer of help with protective equipment like masks, testing kits and medical personnel, world is finding it difficult to hold the grudge against it for violating WHO IHR(2005)(WHO IHR) guidelines, and keeping the world in dark about origin and spread of a potential PHEIC (public health emergencies of international concern) before it became a pandemic. Instead its Wuhan model of control of pandemic is seen as ideal for suppression of the transmission of infection and prompt regress to socio-economic normality.
India has done well in joining the videoconference held by China on COVID-19 lessons and successful combat strategies. Our prime minister’s effort to bring the SAARC nations on one platform to fight the pandemic and the pledge of help other nations in the time of crisis is states manly and strategically apt.
While keeping the universal flight directive of wearing your own mask first before helping others, we must take the lead in production of essential fever & cough medicines, PPE and medical equipment in our readiness for the internal fight and helping the neighbors in time of their crisis. Such an opportunity for good will and friendship must not be frittered.
I conclude by saying these are extraordinary times. With the pandemic unfolding rapidly, information, knowledge, guidance and multilateral collaboration are also becoming available fast for us to fine-tune our combat strategies.
While the politicians have an unenviable responsibility of taking decisions on strategies to control a novel pandemic with no known cure in a period of grave concern and uncertainty, every individual acting preemptively can make huge difference by breaking the chain of transmission. India’s communities have always come together as one to work and assist in times of crisis. I am hopeful that together we shall be able to overcome this one too with minimum loss to life and livelihoods.
(The author worked as Special Secretary, Health & Family Welfare, Commissioner Food and Drugs, Project Director for HIV/AIDS Control for Government of National Capital Territory of Delhi. She is currently studying MSc Economics at University of Texas at Austin, USA, and is certified in Data Analytics from McCombs School, UT Austin. Views expressed are personal)


















Comments
0 comment